TMJ Guide
The Fourth Trimester: What Nobody Tells You About the First 12 Weeks (2026)
The fourth trimester explained — what really happens in the first 12 weeks postpartum, from physical recovery and emotional shifts to newborn needs and partner support. Expert guide by a midwife.
By Dr. Amy W., Midwife & Postnatal Specialist · Published 2026-03-29 · Updated 2026-03-29
The Fourth Trimester: What Nobody Tells You About the First 12 Weeks (2026)
The fourth trimester — the first 12 weeks after birth — is one of the most physically demanding, emotionally intense, and profoundly transformative periods in a woman's life. Yet it is also the phase that receives the least preparation, the least medical attention, and the least honest conversation. Your body is healing from a major medical event, your hormones are in freefall, your baby needs you around the clock, and nobody warned you about half of it. This guide covers what actually happens — and what actually helps.
Affiliate Disclosure: This post contains affiliate links. We may earn a commission at no extra cost to you. See our affiliate disclosure for details.
By Dr. Amy W., Midwife & Postnatal Specialist — Last updated March 2026
Table of Contents
- What Is the Fourth Trimester?
- Physical Recovery: What's Actually Happening to Your Body
- The Emotional Earthquake: Hormones, Identity, and Mental Health
- What Your Newborn Actually Needs (and Doesn't)
- Partner Support: How to Actually Help
- Self-Care That Actually Works (Not Just "Take a Bath")
- Fourth Trimester Essentials: Products Worth Having
- Week-by-Week: What to Expect
- Frequently Asked Questions
- About the Author
- Sources & References
What Is the Fourth Trimester?
The term "fourth trimester" was popularised by paediatrician Dr. Harvey Karp, but the concept has been understood by midwives and postnatal cultures worldwide for centuries. It refers to the first 12 weeks after birth — a period that is physiologically, hormonally, and emotionally as significant as any trimester of pregnancy.
Here's the core truth that Western postnatal care often fails to communicate: birth is not the finish line. It is the start of a recovery process that involves every system in your body.
During pregnancy, your blood volume increased by 50%. Your uterus expanded from the size of a pear to the size of a watermelon. Your ligaments softened, your organs shifted, your pelvic floor bore increasing weight for 40 weeks, and your hormones reached levels hundreds of times their baseline. All of that now has to reverse — while you simultaneously keep a newborn alive on no sleep.
Why Nobody Talks About It
Antenatal care is structured around pregnancy and birth. Postnatal care in most healthcare systems amounts to a single 6-week check-up — and even that appointment is frequently focused on contraception rather than the mother's recovery. The cultural narrative centres the baby's milestones while the mother's experience is reduced to "how are you adjusting?"
This is not a small oversight. The fourth trimester involves:
- Physical recovery from a major medical event (vaginal or surgical)
- Hormonal withdrawal more dramatic than any other life event
- Sleep deprivation at levels that would be considered unsafe in any other context
- Identity transformation — the psychological shift into parenthood
- Relationship recalibration — with your partner, family, and self
- Neurological changes — your brain literally restructures during the postpartum period
For a detailed breakdown of the physical healing journey, see our postpartum recovery week-by-week guide.
Physical Recovery: What's Actually Happening to Your Body
The "6-week recovery" timeline is misleading. Six weeks is the minimum time for basic wound healing and uterine involution. Full musculoskeletal, hormonal, and neurological recovery takes 6–12 months minimum, and some changes (like pelvic floor remodelling) continue for up to 2 years.
Weeks 1–2: Acute Recovery
Lochia (postpartum bleeding): You will bleed for 4–6 weeks regardless of delivery method. The first 2 weeks are heaviest — bright red, potentially with clots. This is your uterus shedding the lining that supported your pregnancy. Use maternity pads (not tampons). Bleeding that soaks a pad in under an hour, or large clots (bigger than a golf ball), requires immediate medical assessment.
Uterine contractions (afterpains): Your uterus contracts to return to its pre-pregnancy size. These are more intense with subsequent births and during breastfeeding (oxytocin triggers contractions). They can be genuinely painful — don't underestimate them.
Perineal recovery: If you had a vaginal birth, perineal soreness (whether from tearing, episiotomy, or simply stretching) is significant. A peri bottle, sitz baths, and witch hazel pads are not luxuries — they are necessities. If you had a C-section, your incision requires careful monitoring for infection (redness, warmth, unusual discharge, fever).
Breast engorgement: Whether or not you breastfeed, your milk will come in around days 2–5. Engorgement can be intensely uncomfortable. For breastfeeding mothers: frequent feeding is the best relief. For those not breastfeeding: cold compresses, supportive bras, and avoiding stimulation will help milk supply decrease.
Night sweats: Postpartum night sweats affect up to 35% of women and are caused by your body eliminating the extra fluid volume from pregnancy. They can be drenching. Layer your bedding and keep spare sheets accessible.
Weeks 3–6: Transition Phase
The acute symptoms begin to ease, but new ones may emerge:
Pelvic floor dysfunction: Urinary leaking, pelvic pressure, or a feeling of heaviness are common — not normal. "Common" and "normal" are different things. These symptoms indicate your pelvic floor needs rehabilitation, not acceptance. Start with gentle pelvic floor exercises (if cleared by your provider) and consider a pelvic floor physiotherapist. See our pelvic floor exercises after birth guide.
Diastasis recti: The separation of abdominal muscles along the midline affects the majority of women postpartum. A gap of 2+ finger-widths at 6 weeks warrants targeted rehabilitation. Avoid sit-ups and planks until assessed. Our diastasis recti guide covers self-assessment and evidence-based exercises.
Back and joint pain: The hormone relaxin (which loosened your ligaments during pregnancy) takes months to clear your system. This means joints remain hypermobile and vulnerable. Combined with the repetitive postures of nursing and carrying, back pain is extremely common.
Constipation: Fear of the first postpartum bowel movement is universal and valid. Stool softeners, adequate hydration, and fibre are your friends. Do not strain.
Weeks 6–12: The "Should Be Better by Now" Phase
This is the period where societal expectations diverge most sharply from biological reality. You're expected to be "back to normal" — but your body is still actively healing.
Hormonal shifts continue: Oestrogen and progesterone remain at lower levels. If breastfeeding, prolactin stays elevated and can suppress your menstrual cycle. The hormonal profile of a woman at 8 weeks postpartum is dramatically different from her non-pregnant baseline.
Hair loss begins: Around 3 months postpartum, the hair that was retained during pregnancy starts to shed — sometimes dramatically. This is telogen effluvium, and it is temporary (though alarming). Read more in our postpartum hair loss guide.
Energy debt accumulates: Three months of sleep deprivation takes a cumulative toll. You may feel worse at 10 weeks than you did at 4 — this is normal and doesn't mean something is wrong. It means sleep deprivation compounds over time, and your body is running on reserves.
Sexual health: Clearance at 6 weeks does not mean readiness. Vaginal dryness (especially if breastfeeding), scar sensitivity, pelvic floor weakness, body image changes, and simple exhaustion all affect sexual desire and comfort. There is no mandatory timeline. Communicate with your partner.
The Emotional Earthquake: Hormones, Identity, and Mental Health
The emotional reality of the fourth trimester is under-discussed to a degree that borders on negligent. Preparing women for birth but not for the psychological aftermath is like training someone to run a marathon and then abandoning them at the finish line with no water, no directions, and no ride home.
Baby Blues vs. Something More
Baby blues affect 50–80% of new mothers and typically appear within the first 2 weeks. Symptoms include tearfulness, mood swings, irritability, and feeling overwhelmed. Baby blues resolve on their own by 2–3 weeks postpartum.
If symptoms persist beyond 2 weeks, intensify rather than improve, or include thoughts of self-harm — this is not baby blues. This may be postpartum depression or postpartum anxiety, both of which are clinical conditions requiring treatment. For a thorough comparison of these conditions, see our guide on postpartum anxiety vs depression.
The Hormonal Cliff
Within the first 24–48 hours after delivery, your oestrogen and progesterone levels drop precipitously — from the highest levels they will ever be to near-zero. This is the largest hormonal shift in human physiology. For context: the hormonal withdrawal after birth is more dramatic than menopause, which unfolds over years rather than hours.
This hormonal cliff affects:
- Mood regulation — serotonin and dopamine pathways are disrupted
- Sleep architecture — even when you can sleep, your sleep quality is altered
- Thermoregulation — hot flashes, night sweats, chills
- Cognitive function — "mum brain" is a real neurological phenomenon, not laziness
- Libido — suppressed by low oestrogen and high prolactin
Matrescence: The Identity Shift
Reproductive psychologist Aurelie Athan coined the term "matrescence" to describe the developmental process of becoming a mother — a transition as significant as adolescence. Just as adolescence involves identity confusion, mood instability, and physical change, so does matrescence.
You may experience:
- Grief for your pre-baby identity, body, freedom, or career trajectory
- Ambivalence about motherhood (loving your baby and hating aspects of new parenthood are not mutually exclusive)
- Rage — postpartum anger is underdiagnosed and often a symptom of anxiety or depression
- Hypervigilance — a biologically driven state where you are physiologically wired to perceive threats to your baby
- Loneliness — despite being with your baby 24/7, the isolation of early postpartum is profound
When to Get Help
You should seek professional support if:
- Sadness, anxiety, or anger persist beyond 2 weeks
- You have intrusive thoughts that frighten you
- You cannot sleep even when the baby is sleeping
- You feel disconnected from your baby
- You are unable to eat or care for yourself
- You have thoughts of harming yourself or your baby (call 988 or PSI: 1-800-944-4773 immediately)
Postpartum mood disorders are treatable — and treatment works. CBT, medication (safe during breastfeeding), and peer support are all evidence-based interventions.
What Your Newborn Actually Needs (and Doesn't)
Your baby has just transitioned from the most consistent, controlled environment possible — your uterus — to a world of bright lights, cold air, open space, and unpredictable sounds. Understanding this helps explain virtually every "difficult" newborn behaviour in the first 12 weeks.
What Newborns Need
Physical closeness. This is not a preference — it is a physiological need. Skin-to-skin contact regulates newborn heart rate, breathing, temperature, and blood sugar. Babies who are held more cry less (research consistently demonstrates this). You cannot "spoil" a newborn.
Feeding on demand. Whether breast or bottle, newborns feed frequently — often 8–12 times in 24 hours, with cluster feeding periods where they feed almost continuously for hours. This is normal. During growth spurts (around days 7–10, 3 weeks, 6 weeks, and 3 months), feeding frequency increases further.
Sleep support. Newborns sleep 14–17 hours per day but in short bursts of 2–4 hours. They do not have circadian rhythm — day and night mean nothing to them until around 6–8 weeks when melatonin production begins. Sleep will not consolidate until 3–4 months at the earliest.
Sensory familiarity. White noise mimics the sound environment of the womb (which is louder than a vacuum cleaner). Swaddling mimics the containment they experienced in utero. Gentle motion recreates the movement of being carried during pregnancy. These are not "crutches" — they are developmentally appropriate comfort measures.
What Newborns Don't Need
- Stimulation overload. Newborns are easily overstimulated. They don't need toys, classes, or social events. They need you.
- A perfect schedule. Newborn schedules are meaningless until circadian rhythm develops. Follow your baby's cues, not a clock.
- Visitors on demand. Your baby doesn't need to "meet everyone." Visitors should serve the parents, not the other way around.
- A perfectly quiet house. Newborns are accustomed to constant noise. Ambient sound is fine. Tiptoeing creates light sleepers.
Colic, Witching Hours, and Cluster Feeding
The late afternoon/evening "witching hour" (typically 5–10 PM) when your baby is fussy, inconsolable, and wants to feed constantly is one of the most exhausting fourth-trimester experiences. It is normal, peaks around 6 weeks, and gradually resolves by 3–4 months.
True colic (defined as crying for 3+ hours, 3+ days per week, for 3+ weeks) affects approximately 10–25% of newborns. It is not caused by something you're doing wrong. It is not fully understood, resolves on its own, and the best strategy is survival: take shifts with your partner, use motion (car rides, stroller walks), and know that it will pass.
Partner Support: How to Actually Help
If you are the partner of someone in the fourth trimester, the single most important thing you can read is this: your primary job right now is not bonding with the baby. Your primary job is protecting the recovery of the person who gave birth.
This is not to diminish the partner-baby relationship — it matters enormously. But the birthing parent has had a major medical event and needs recovery conditions. The baby needs a recovering parent to survive.
The Practical Essentials
Protect sleep. This is the single highest-impact intervention. Take the baby between feeds so the birthing parent can sleep in 3–4 hour uninterrupted blocks. If breastfeeding, bring the baby for feeds and then take baby back for settling. Even one protected sleep block per 24 hours significantly reduces postpartum depression risk.
Own the household. Cooking, cleaning, laundry, dishes, groceries, pet care, older children — these are your domain now. Don't ask "what needs doing" — look around and do it. The cognitive load of delegating household tasks is itself exhausting.
Manage visitors. Be the gatekeeper. Visitors should be brief, bring food, and help — not create hosting obligations. It is your job to say "we're not taking visitors this week" so the birthing parent doesn't have to be the bad guy.
Track warning signs. You are in a better position than anyone to notice changes in your partner's mood, behaviour, or functioning. Persistent crying, withdrawal, inability to sleep even when the baby is asleep, expressions of hopelessness, or statements like "the baby would be better off without me" require immediate professional intervention.
What Not to Do
- Don't say "you should sleep when the baby sleeps" (this is rarely possible and dismissive of reality)
- Don't compare their recovery to anyone else's
- Don't suggest they're "overreacting" to physical symptoms
- Don't wait to be asked — anticipate needs
- Don't treat caring for your own baby as "babysitting" or "helping out"
- Don't disappear into work, hobbies, or screens to cope with the stress — you are needed present
Partners Have Feelings Too
This section would be incomplete without acknowledging that partners also undergo a psychological transition. Paternal/partner postpartum depression affects approximately 10% of new fathers. Feeling helpless, shut out, overwhelmed, or resentful does not make you a bad partner. It makes you human. Seek support — from friends, from your own provider, from PSI's partner resources.
Self-Care That Actually Works (Not Just "Take a Bath")
The "self-care" messaging directed at new mothers is often unhelpful — it suggests elaborate routines that require time and energy you don't have, and it implies that your distress is a personal failure to "take care of yourself" rather than a systemic failure to support postpartum recovery.
Real fourth-trimester self-care is unglamorous. It is the basics, done consistently.
Sleep
Sleep is not optional wellness — it is a medical necessity for recovery. Every system in your body that is healing requires sleep to do so. Prioritise sleep above everything except feeding your baby and basic safety.
Strategies:
- Sleep when someone else can take the baby — even if it's "not bedtime"
- Accept help from anyone offering it, specifically for the purpose of sleeping
- If you cannot sleep even when the opportunity arises, tell your provider — insomnia despite exhaustion is a red flag for postpartum anxiety
Nutrition
You are recovering from a major physical event and potentially producing breast milk (which requires an additional 300–500 calories daily). This is not the time for restrictive eating.
- Eat enough. Aim for regular, protein-rich meals.
- Hydrate aggressively. Especially if breastfeeding — keep a large water bottle within reach at all times.
- Accept meal trains. If friends or family offer to cook, say yes. If nobody offers, services like frozen meal delivery exist.
- Supplement where needed. Postnatal vitamins, iron (if levels are low — common after blood loss during delivery), vitamin D, and omega-3s all have evidence-based roles in postpartum recovery.
Movement
Don't exercise "to get your body back." Move because gentle movement supports healing, reduces depression risk, and helps with constipation and joint stiffness.
- Weeks 1–2: Short walks around the house
- Weeks 2–6: Gentle walks outside (weather and energy permitting)
- After 6-week clearance: Gradual return to activity, ideally guided by a postpartum-trained physiotherapist
- Avoid high-impact exercise until pelvic floor is assessed
Lowering the Bar
The most effective self-care strategy in the fourth trimester is reducing demands. Lower your standards for housekeeping. Say no to obligations. Postpone decisions that can wait. Unfollow social media accounts that make you feel inadequate. Your only job right now is recovering and keeping your baby alive. Everything else can wait.
Fourth Trimester Essentials: Products Worth Having
Frida Mom Postpartum Recovery Essentials Kit
Best for: Complete perineal recovery — peri bottle, cooling liners, disposable underwear
Why it matters: Hospital supplies run out fast; this kit covers weeks 1–3 comfortably
Rating: 4.7/5 (12,000+ reviews)
Price: $$
Check on Amazon →
Haakaa Silicone Breast Pump — Manual Milk Collector
Best for: Catching letdown from the non-nursing side, building a small stash without pumping
Why it matters: Effortless, no-power milk collection that doesn't increase supply beyond needs
Rating: 4.8/5 (45,000+ reviews)
Price: $
Check on Amazon →
Belly Bandit Original Belly Wrap
Best for: Abdominal support, C-section incision comfort, diastasis recti compression
Why it matters: Gentle compression reduces swelling and provides core stability when muscles are weakest
Rating: 4.5/5 (8,000+ reviews)
Price: $$
Check on Amazon →
Hatch Rest Sound Machine — Nursery Essential
Best for: White noise for newborn sleep, nightlight for night feeds, sleep cue routine
Why it matters: Mimics womb sounds, helps newborn (and you) sleep longer stretches
Rating: 4.7/5 (30,000+ reviews)
Price: $$
Check on Amazon →
Ergobaby Embrace Newborn Carrier
Best for: Hands-free holding, reducing crying, enabling movement while meeting baby's contact needs
Why it matters: Babywearing meets your newborn's need for closeness while freeing your hands
Rating: 4.6/5 (5,000+ reviews)
Price: $$
Check on Amazon →
Stanley 40oz Insulated Tumbler — Hydration Essential
Best for: Keeping water accessible during nursing sessions, one-handed drinking
Why it matters: Dehydration worsens fatigue, constipation, and milk supply — a large tumbler by your nursing station is non-negotiable
Rating: 4.8/5 (100,000+ reviews)
Price: $
Check on Amazon →Week-by-Week: What to Expect
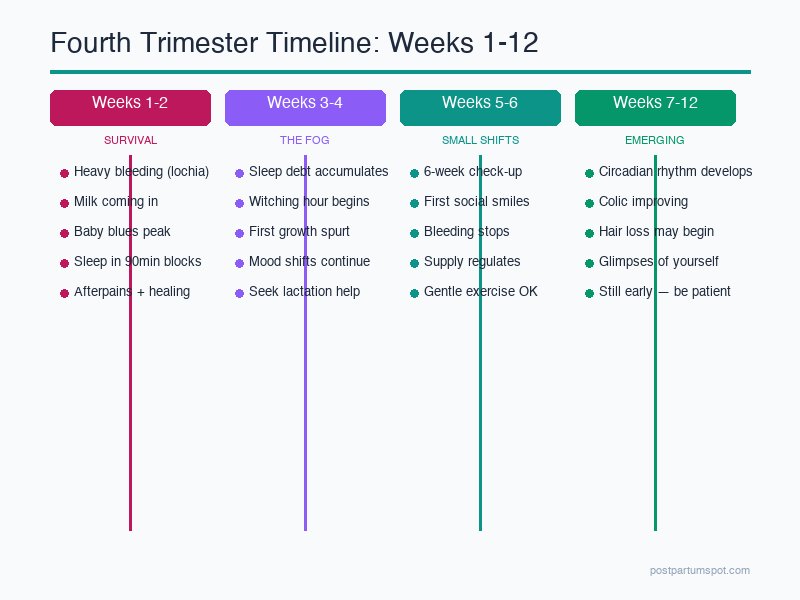
Weeks 1–2: Survival Mode
- Heaviest postpartum bleeding
- Milk coming in (days 2–5), potential engorgement
- Intense afterpains (especially with breastfeeding)
- Baby blues peak (days 3–5)
- Baby feeding every 1.5–3 hours around the clock
- Sleep measured in 90-minute increments
- Your only goals: Feed baby. Feed yourself. Sleep when possible. Accept help.
Weeks 3–4: The Fog
- Bleeding transitions from red to pink/brown
- Sleep deprivation accumulates — this is often the hardest period
- Baby may become more alert and fussy (the witching hour begins)
- Breastfeeding may still be painful — this is not automatically normal. Seek lactation support.
- Hormonal mood swings either begin to stabilise or become a pattern (watch for persistent symptoms)
- First growth spurt around 3 weeks — increased fussiness and feeding
Weeks 5–6: Small Shifts
- 6-week postnatal check-up — advocate for yourself. Ask about pelvic floor, mood, pain, and any concerns.
- Baby may begin social smiling — this is neurologically significant and genuinely transformative for bonding
- Bleeding typically stops or nearly stops
- Energy may improve slightly — or may not. Both are normal.
- If breastfeeding, supply typically regulates around this time
- Clearance for gentle exercise and (potentially) intercourse — but clearance ≠ readiness
Weeks 7–8: Emerging Patterns
- Baby's circadian rhythm begins to develop — you may notice longer nighttime sleep stretches
- Feeding patterns may become slightly more predictable
- Your body has completed basic wound healing
- Risk period for postpartum mood disorders continues — don't dismiss persistent symptoms because "it should be better by now"
Weeks 9–12: The Home Stretch
- Baby becomes significantly more interactive, alert, and social
- Colic and witching hour behaviour typically peaks at 6 weeks and is improving by 10–12 weeks
- You may begin to feel glimpses of yourself again — interspersed with exhaustion
- Hair loss may begin (telogen effluvium, peaking around 3–4 months)
- Many parents return to work during this period — the emotional complexity of this transition is underestimated
- Important: Feeling like you "should" be recovered but aren't is common. Twelve weeks is still early.
For a more detailed week-by-week physical recovery timeline, see our comprehensive postpartum recovery guide.
Frequently Asked Questions
What is the fourth trimester? The fourth trimester refers to the first 12 weeks (approximately 3 months) after birth. It's a period of profound adjustment for both the birthing parent and baby — physically, emotionally, and hormonally. The term recognises that birth is not the end of a process but the beginning of a new, equally demanding phase.
How long does the fourth trimester last? The fourth trimester lasts approximately 12 weeks (3 months) after birth. However, full postpartum recovery can take 6–12 months or longer. The 12-week mark is significant because it's when many physical and hormonal changes begin to stabilise and when most newborns start showing more predictable patterns.
Is it normal to feel overwhelmed during the fourth trimester? Yes — feeling overwhelmed during the fourth trimester is extremely common and not a sign of failure. Sleep deprivation, hormonal shifts, physical recovery, and the adjustment to 24/7 caregiving combine to create a uniquely challenging period. However, if feelings of overwhelm persist beyond 2 weeks, interfere with daily functioning, or include thoughts of self-harm, seek professional support immediately.
When should I see a doctor during the fourth trimester? See a healthcare provider if you experience: heavy bleeding that soaks a pad in under an hour, fever above 100.4°F (38°C), signs of wound infection, persistent sadness or anxiety lasting more than 2 weeks, inability to care for yourself or your baby, or thoughts of harming yourself or your baby. Don't wait for the 6-week check-up if something feels wrong.
How can partners help during the fourth trimester? Partners can help by handling household tasks, managing visitors, protecting the birthing parent's sleep by taking baby between feeds, attending postpartum appointments together, watching for signs of postpartum depression or anxiety, and providing emotional support without judgment. The single most impactful thing a partner can do is protect uninterrupted sleep blocks of 3–4 hours.
What are the most common fourth trimester physical symptoms? Common physical symptoms include lochia (postpartum bleeding lasting 4–6 weeks), perineal soreness, breast engorgement, night sweats, hair shedding (typically starting around 3 months), abdominal separation (diastasis recti), back pain, and fatigue. Most of these gradually improve over the 12-week period with appropriate rest and care.
About the Author
Dr. Amy W. is a certified nurse-midwife and postnatal specialist with over 15 years of experience supporting women through pregnancy, birth, and the postpartum period. She is a Fellow of the American College of Nurse-Midwives (ACNM) and specialises in fourth-trimester recovery, perinatal mental health screening, and evidence-based postnatal care. She is a strong advocate for extending postpartum medical support beyond the standard 6-week check-up.
Sources and References
- Karp, H. The Happiest Baby on the Block, 5th ed. Bantam, 2015. (Origin of the "fourth trimester" concept in popular discourse.)
- Romano, M., Cacciatore, A., et al. "Postpartum period: three distinct but continuous phases." Journal of Prenatal Medicine, 2010. PMID: 22439056
- Athan, A.M. "Reproductive identity: An emerging concept." American Psychologist, 2020. DOI: 10.1037/amp0000456 (Matrescence framework.)
- O'Hara, M.W., Wisner, K.L. "Perinatal mental illness: definition, description and aetiology." Best Practice & Research Clinical Obstetrics & Gynaecology, 2014. DOI: 10.1016/j.bpobgyn.2013.09.002
- Postpartum Support International (PSI). Helpline: 1-800-944-4773. Resources and provider directory at postpartum.net.
- American College of Obstetricians and Gynecologists (ACOG). "Optimizing Postpartum Care." Committee Opinion No. 736, 2018 (reaffirmed 2024).
- Dennis, C.L., Dowswell, T. "Psychosocial and psychological interventions for preventing postpartum depression." Cochrane Database of Systematic Reviews, 2013.
Crisis Resources:
- Postpartum Support International Helpline: 1-800-944-4773
- National Suicide Prevention Lifeline: 988
- Crisis Text Line: Text HOME to 741741
This article is for informational purposes only and does not constitute medical advice. If you are experiencing postpartum symptoms that concern you, please consult a qualified healthcare provider.
Walking Pad vs Treadmill
30-second comparison